

Background
The most common cause of severe renal impairment in myeloma (MM) is the direct effect of a high concentration of nephrotoxic monoclonal free light chains (LC) leading to MM cast nephropathy. Decreasing LC and therefore improving renal function is important for long term outcome.
In the UK NCRI Myeloma XI trial the addition of the second generation PI carfilzomib (K) to the immunomodulatory agent (IMiD) lenalidomide, cyclophosphamide and dexamethasone (Rdc) improved progression-free survival (PFS) in newly diagnosed MM patients (NDMM) eligible for autologous stem cell transplant (ASCT) (median PFS KRdc not reached (NR) v Rdc 36 months HR 0.66 (95% CI 0.52, 0.83, P=0.0004). This exploratory subgroup analysis compares PFS and renal recovery between patients receiving KRdc and Rdc within renal function subgroups.
Methods
Myeloma XI is a phase III, randomized controlled trial with an adaptive design for symptomatic NDMM patients of all ages. This renal analysis is of the transplant eligible (TE) pathway and compares induction treatment with the quadruplet KRdc to triplet Rdc. Patients were randomized contemporaneously 2:1. All patients were randomized to post-ASCT R maintenance or observation. For further exploratory analysis patients randomized earlier in the study to Rdc were also included.
Relevant exclusion criteria were acute renal failure non-responsive to 72 hours rehydration (creatinine >500umol/L, urine output <400ml/day or dialysis). The Modification of Diet in Renal Disease formula was used to calculate the baseline estimated glomerular filtration rate (eGFR). Renal function was normal, eGFR >=60 ml/min/1.73m2, moderately impaired 30-59 or severely impaired <30. Potentially nephrotoxic LC were considered those with a difference of >=500mg/L between the involved and uninvolved (dFLC). Renal recovery was defined as an improvement in eGFR of ≥25% at the end of induction therapy.
Results
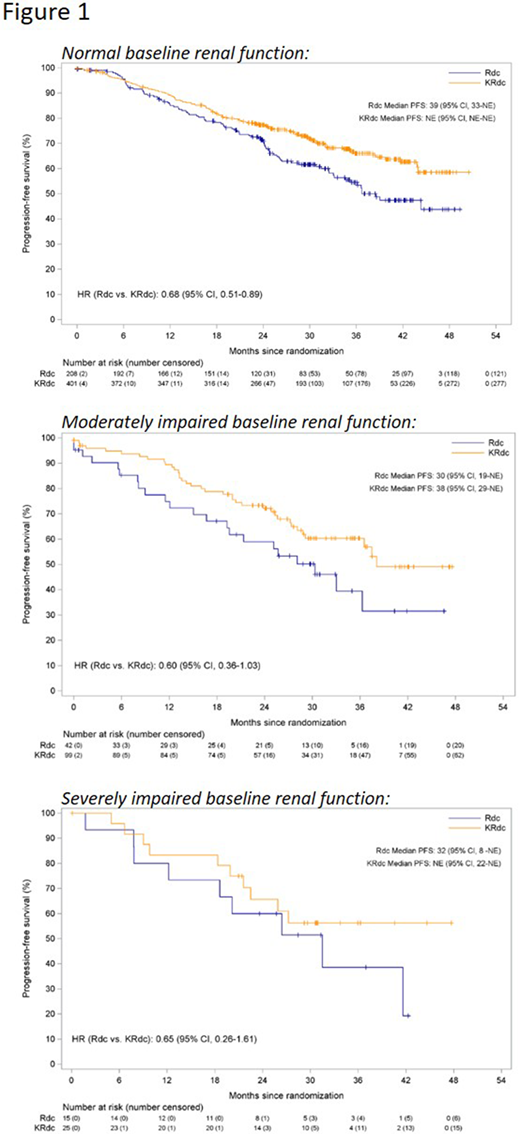
1547 patients were randomized to KRdc n=526 or Rdc n=1021 (265 contemporaneous, 756 not). In the contemporaneous group baseline renal function was normal in 609/791 (77.0%), moderately impaired in 141/791 (17.8%) and severely impaired in 40/791 (5.1%) (data n/a in 1 patient). Patients with moderately or severely impaired renal function had shorter PFS compared to those with normal renal function. Subgroup analysis showed consistent outcomes for KRdc compared to Rdc across all renal subgroups with no evidence of significant heterogeneity (Figure 1, Phet=0.9354).
Further exploratory analysis combined patients with moderate or severe renal impairment into one group. Difference in PFS and renal recovery between patients with normal or impaired renal function and high (>=500) or low (<500) dFLC were examined. Consistent with the findings in the contemporaneous group, KRdc was associated with a significant improvement in PFS compared to Rdc in both the normal and renal function impaired groups.
Within the group of patients with normal renal function at baseline those with high dFLC had shorter PFS than those with low dFLC. KRdc was associated with improved PFS irrespective of LC level: high dFLC KRdc median PFS NR (95% CI 39, NR) v Rdc 34 months (30, 39) and low dFLC KRdc NR (44, NR) v Rdc 41 (37, 47).
In the group of patients with renal impairment at baseline KRdc was also associated with an improved PFS irrespective of LC level: high dFLC KRdc median PFS NR (95% CI 29, NR) v Rdc 32 months (28, 42) and low dFLC KRdc 37 (25, NR) v Rdc 27 (24, 33). In contrast to those with normal renal function, however, patients with renal impairment and high dFLC had a longer PFS than those with low dFLC. This observation was apparent whether patients received KRdc or Rdc and suggests that patients with high dFLC may have had reversible renal impairment, improving their ultimate outcomes. Supporting this hypothesis, measurable renal recovery in the renal impaired group at the end of induction was more common in patients with high dFLC (dFLC>=500 68.6% v dFLC<500 53.2%). Interestingly the rate of renal recovery was similar between KRdc and Rdc in the high dFLC group (KRdc 71.1% v Rdc 67.5%) suggesting the improved PFS seen with KRdc in the group with renal impairment is not due to an increased rate of renal recovery.
Conclusions
KRdc was associated with improved PFS compared to Rdc in NDMM patients across all renal subgroups. Irrespective of treatment, renal function is more likely to improve if attributable to nephrotoxic LC.
Pawlyn:Janssen: Honoraria, Other: Travel expenses; Celgene: Consultancy, Honoraria, Other: Travel expenses; Amgen: Consultancy, Other: Travel expenses; Takeda: Consultancy, Other: Travel expenses. Menzies:Celgene, Amgen, Merck: Research Funding. Davies:Sanofi: Honoraria, Membership on an entity's Board of Directors or advisory committees; Oncopeptides: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Adaptive Biotech: Honoraria; Celgene/BMS: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding. Cook:Celgene, Janssen, Takeda: Research Funding; Amgen, Bristol-Myers Squibb, Celgene, Janssen, Takeda, Roche, Sanofi: Honoraria; Karyopharm: Honoraria. Gregory:Celgene, Amgen, Merck: Research Funding; Janssen: Honoraria; Celgene: Consultancy. Jenner:Amgen, Janssen, Celgene, Takeda, Novartis, Sanofi, GSK: Consultancy; Janssen, Takeda, Amgen, Celgene, Novartis: Honoraria; Janssen, Celgene: Research Funding; Janssen, Takeda, Amgen: Other: Travel expenses. Jones:Celgene: Honoraria, Research Funding. Kaiser:Bristol-Myers Squibb/Celgene, Janssen, Karyopharm: Research Funding; Bristol-Myers Squibb, Chugai, Janssen, Amgen, Takeda, Celgene, AbbVie, Karyopharm, GlaxoSmithKline: Consultancy; Janssen, Amgen, Celgene, Bristol-Myers Squibb, Takeda: Honoraria; Bristol-Myers Squibb, Takeda: Other: Travel expenses. Owen:Takeda: Honoraria, Other: Travel expenses; Janssen: Consultancy, Other: Travel expenses; Celgene: Consultancy, Honoraria, Research Funding. Morgan:Karyopharm: Consultancy, Honoraria; Janssen: Research Funding; GSK: Consultancy, Honoraria; Bristol-Myers Squibb: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding; Roche: Consultancy, Honoraria; Amgen: Consultancy, Honoraria. Jackson:Takeda: Honoraria, Research Funding, Speakers Bureau; Gsk: Honoraria, Speakers Bureau; Amgen: Honoraria, Speakers Bureau; Janssen: Honoraria, Speakers Bureau; Celgene: Honoraria, Research Funding, Speakers Bureau. Cairns:Celgene, Amgen, Merck: Research Funding; Celgene: Other: Travel Support.
Carfilzomib, lenalidomide, dexamethasone and cyclophosphamide combination induction therapy for newly diagnosed myeloma

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal